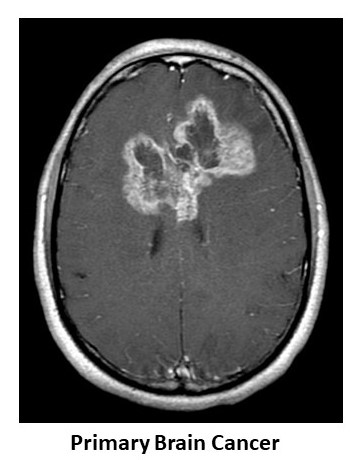
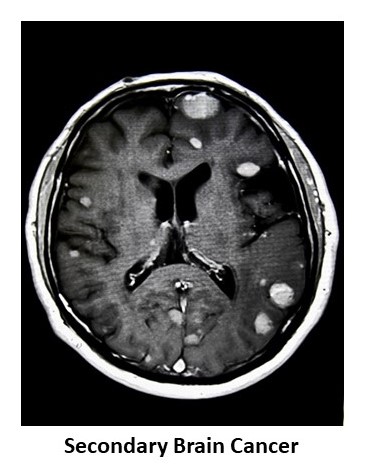
Some brain tumours are found in areas of the brain that control speech, language or even motor control of your arms and legs. These tumours can be both primary (especially for Diffuse Low Grade Gliomas or DLGG) or secondary brain tumours. Our institute specialises in the removal of such tumours by performing brain mapping or awake brain surgery (also known as awake craniotomy).
Brain mapping and awake craniotomy allow brain tumours to be removed while preserving important functions such as language, fine motor skills and executive functions.
For tumours such as DLGG, awake surgery allows for maximal surgical resection of the tumour whilst preserving patients' neurological functions. It is now the standard practice. The aim of early maximal surgical resection of DLGG is not only oncological (i.e. remove as much tumour as safely possible) but just as importantly, to improve the patient's quality of life (in terms of both symptoms and seizure control). Many studies have shown improvements in neuropsychological and functional status as demonstrated by post-operative evaluations, and also improvements in epilepsy control, post resection under awake conditions.
In addition, contrary to belief, patients tolerate the awake procedure well. The brain cannot feel pain. During surgery, functions (such as speech, language and movement) can be tested and patients can provide real-time feedback to the neurosurgeon as the tumour is being excised. This allows the neurosurgeon to safely remove more of the tumour whilst preserving the patient's functions.
Prior to the surgery, the patient will be reviewed yby a team of specialists involved in the awake surgery, namely the neurosurgeon, neuroanaesthetist and neuropsychologist.
The neuroanaesthetist will discuss with the patient about any past medical problems and examine the patient. The whole process of sedation required during the more uncomfortable phases of the surgery (the drilling of the skull and insertion of intravenous cannulae, urine catheter insertion, etc) will also be explained. The patient might experience some headaches and muscle pain from lying in the same position for several hours.
The neuropsychologist will perform a pre-operative neuropsychological assessment that includes a comprehensive characterisation of the patient's cognitive status and evaluation of emotional functioning (e.g. acceptance of diagnosis and treatment, and coping mechanisms). Supportive counselling and psychoeducation will be conducted in the session as well, for the patient and the family where appropriate. Following that, training of the tasks to be done intra-operatively during the awake phase of the surgery will commence.
This is routinely done at the pre-treatment stage and is an integral part of individualised management of patients undergoing awake surgery to have their tumour removed. This evaluation allows characterisation of the patient's baseline functioning, identification of subtle cognitive deficits and planning for post-treatment rehabilitation.
Post-operatively, patients would undergo an individually-tailored rehabilitation programme consisting of physiotherapy, speech and language therapy, as well as other services as required (e.g. supportive counselling, neurocognitive rehabilitation, return-to-work/school support).
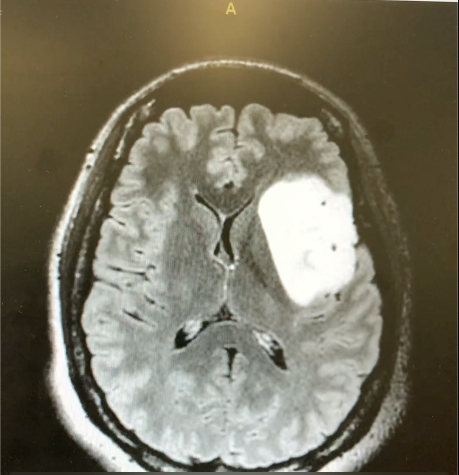
MRI image of a left insular diffuse low grade glioma
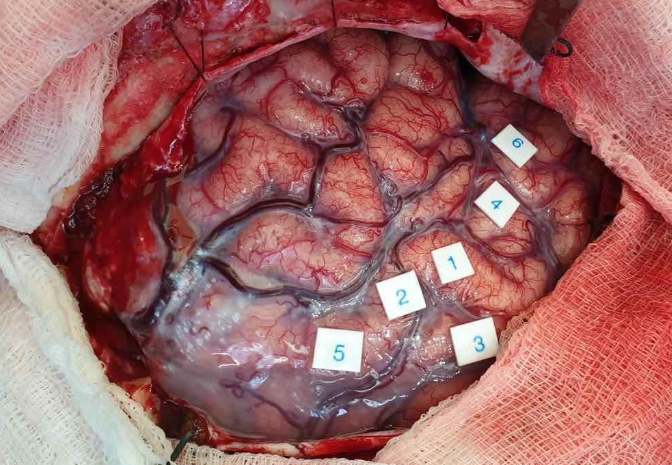
Intraoperative photo of brain mapping (labels indicate eloquent areas of the brain)