Delivery of successful radiation therapy requires the coordinated efforts of a dedicated team of staff with different skill sets.
Our Radiation Oncology Team comprises:
- Radiation Oncologists
- Radiation Therapists
- Medical Physicists
- Radiation Oncology Nurses
- Patient Care Associates and Patient Service Associates
Radiation Oncologists
Radiation oncologists are medical specialists who are qualified to give radiation therapy. The radiation oncologist’s role is to determine the suitability of radiation therapy for each patient, and to give the final approval for the radiation therapy plan. During the course of treatment, the radiation oncologist is also responsible for reviewing patients for side effects. After treatment is completed, the radiation oncologist determines the frequency of follow-up and subsequent tests.
Our radiation oncologists are also actively engaged in undergraduate and post-graduate teaching, as well as clinical research.
RESIDENT PHYSICIAN/REGISTRAR/CLINICAL ASSOCIATE
Dr Katherine Meng Tian
Dr Syadwa A Shukor
Dr Teri Danielle Yeoh
Dr Sreyes Ravi
Dr Wei Wei
Dr Caryn Wujanto
Dr Ye Chen'En
Dr Yip Pui Lam
Radiation Therapists

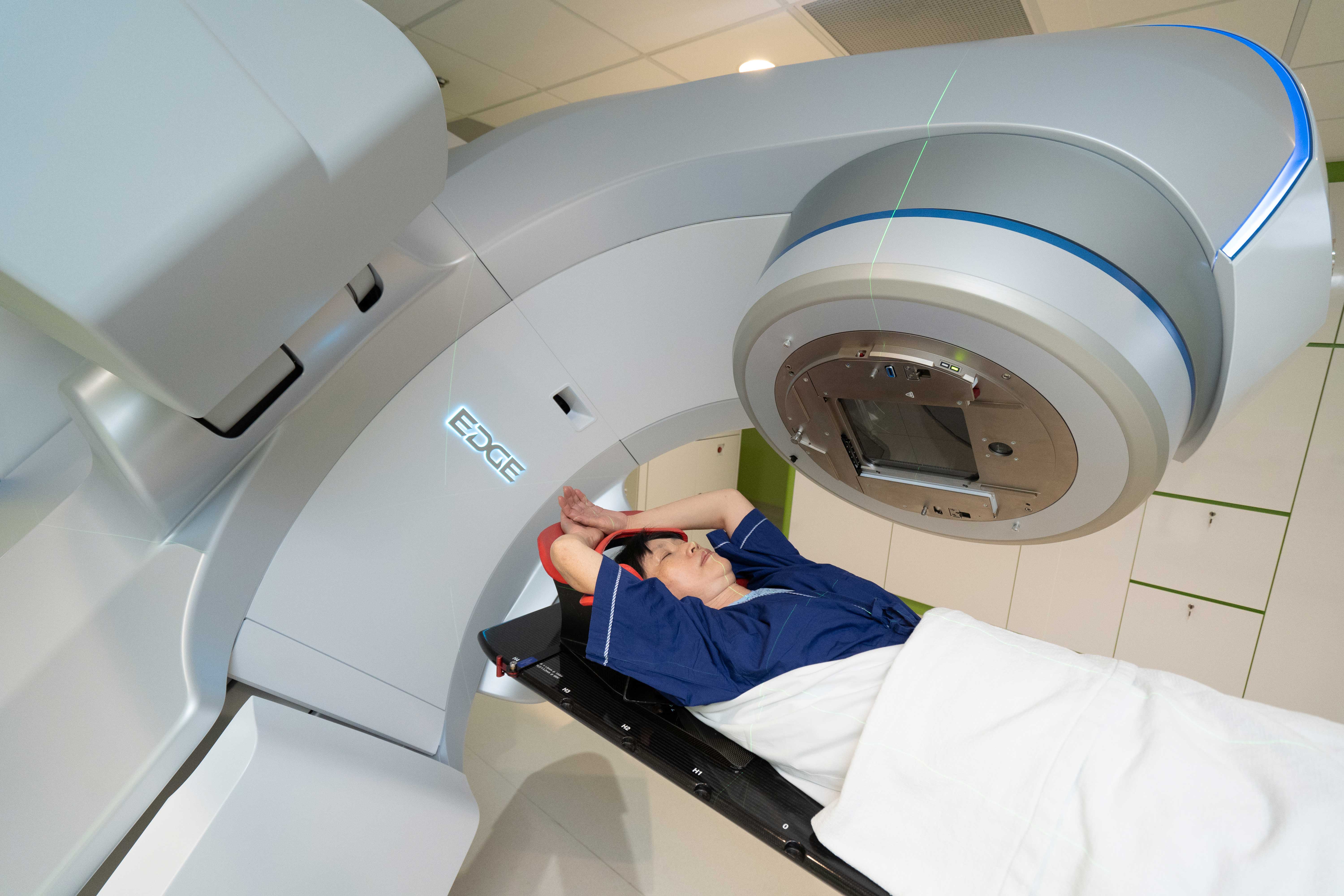
Radiation therapists are a group of allied health professionals who are trained to operate the various systems required in the delivery of radiation therapy to our patients. These systems include data acquisition systems like CT simulation, planning systems for designing radiation therapy plans, as well as treatment units like linear accelerators that ultimately carry out the treatment.
The specific duties of Radiation Therapists include:
- Fabricating immobilisation devices for accurate treatment delivery
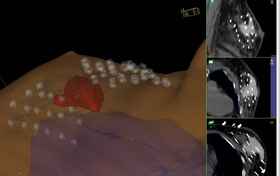
- Simulation for tumour localisation and planning through the use of imaging modalities such as Computed Tomography
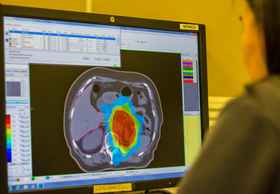
- Designing of treatment plans and dose calculations in collaboration with radiation oncologists and physicists
- Reviewing of prescriptions, images and approved treatment plans to ensure that the information is valid before treatment delivery
- Ensuring daily set-up reproducibility for safe and accurate treatment delivery
- Delivering of radiation treatment and monitoring of patient's condition during treatment delivery
- Advising patients on pre-treatment preparation, procedures and possible side effects of radiation treatment
Radiation Therapists also play an important role in clinical research and implementation of new techniques and protocols in cancer treatment to provide holistic care to our patients.
HEAD, RADIATION THERAPY |
|---|
|
SENIOR PRINCIPAL RADIATION THERAPIST
|
|---|
- Ms Mary Chan
- Ms Yvonne Loh
- Ms Tan Chek Wee
| - Ms Joyce Tan
- Mr John Villalon
|
PRINCIPAL RADIATION THERAPIST
|
|---|
- Ms Wendy Hoy
- Ms Samatha Koh
| - Ms Darcy Yeo
- Ms Sarahatul Yusoff
|
SENIOR RADIATION THERAPIST
|
|---|
- Ms Richerlyn Beltran
- Mr Cai Shao Bin
- Ms Tabitha Chan
- Ms Desiree Chen
- Ms Serene Cher
- Ms Clara Chew
- Ms Corin Chng
- Mr Jeremy Chong
- Mr Guo Weiguang
- Mr Mohd Hafiz
- Mr Muhammad Haziq
- Ms Carinne Ho
- Mr Ho Guan Da
- Ms Esperanza Humigop
- Ms Kang Chern Lynn
- Mr Koh Guan Lee
| - Mr Mark Lawrence
- Ms Liang Jun
- Ms Shana Lee
- Ms Leong Manling
- Ms Michelle Muhundan
- Ms Vanishree Naidu
- Ms Jessie Ng
- Ms Ngean Ai Geok
- Mr Ong Kok Chuan
- Mr Muhammad Rahmatullah
- Mr Xavier Selvanathan
- Ms Wennie Song
- Ms Teng Kie Yin
- Ms Yeo Li Wen
- Mr Zheng Jian Yong
|
RADIATION THERAPIST
|
|---|
- Mr Cheow Min Wah
- Ms Lee Xin Min
- Ms Nur Fathiah Abdul Razak
- Ms On Chin Leng
- Ms Jaslyn Tan
| - Ms Jolina Tan
- Ms Tan Zu Qi
- Ms Eunice Wijeysingha
- Mr Zhang Bonan
|
Medical Physicists
Medical physicists provide the scientific and technical support in a radiation oncology department. They assist in creating, implementing and monitoring the procedures which allow the best treatment using radiation, taking into account the protection and safety of patients and others involved in the treatment process.
Medical physicists make sure that all equipment meet international and national standards. This can include machines such as linear accelerators, CT scanners, treatment computer systems and radioactive materials. They are also responsible for the design of new radiation oncology facilities and the commissioning of new equipment.
Medical physicists train other professional groups on topics such as radiation physics and radiation safety. They also have both a primary and supporting role in research activities in a radiation oncology department.
CHIEF MEDICAL PHYSICIST |
|---|
|
SENIOR PRINCIPAL RADIATION PHYSICIST
|
|---|
|
SENIOR RADIATION PHYSICIST
|
|---|
- Ms Joan Faith Loria
- Ms Leong Yun Fun
- Ms Teh Mun Woan
|
RADIATION PHYSICIST
|
|---|
- Mr Khor Jong Shin
- Mr Jessen How
|
Radiation Oncology Nurses

Radiation Oncology Nurses are licensed registered nurses who work collaboratively with radiation oncologists and radiation therapists to care for patients at the time of initial consultation, during radiation treatment, and at follow-up appointments.
Our nurses provide the following important functions leading up to a patient's successful treatment:
Symptom Management and Patient Education
Prior to the initiation of radiation therapy, radiation oncology nurses provide counseling for patients and their caregivers on the possible side effects of treatment they may experience. During radiation therapy, they will assess patients for ongoing toxicity and advise them on appropriate nursing care. Where necessary, they may also actively manage the symptoms, for instance, applying necessary dressing to skin affected by radiation therapy.
Assistance in Medical Procedures
Sometimes, radiation therapy may involve specialised procedures requiring placement of applicators, sedation or clinical monitoring. In these instances, our nurses are often called upon to assist the radiation Oncologist to ensure the procedures are done effectively and safely.
Emotional Support
Recognising that the period of radiation therapy can be a difficult time for patients and their loved ones, our nurses are available to provide support and counseling. They can help patients access various community resources and support groups, as well as assist with issues such as home care, hospice or medical equipment.
Patient Care Associates and Patient Service Associates

Patient Care Associates (PCAs) and Patient Service Associates (PSAs) are ancillary staff who play key roles in the coordination of patient care and general administration.
They are responsible for the registration of patients upon arrival, handling of appointments and assisting the doctor during consultation. When a decision is made for radiation therapy, they will provide the necessary financial counseling before treatment is initiated. Our PCAs and PSAs work closely with the different teams in the Radiation Therapy Centre to help create a better experience for our patients.
PATIENT SERVICE COORDINATOR |
|---|
|
SENIOR PATIENT SERVICE ASSOCIATE |
|---|
- Ms Arifah Binte Hussein
- Ms Ong Gek Ting
- Ms Noratiqah Binte Hassan
|
PATIENT SERVICE ASSOCIATE |
|---|
- Ms Lee Wan Jing
- Ms Ho Poh Geck
| - Ms Ong Ee Hui
- Ms Sanjeeta Devi D/O Rajasingam
|